Forward Looking Post - What does Summer Look Like?
- Erin Bromage

- Apr 24, 2020
- 9 min read
Updated: Dec 28, 2021
A few weeks ago, I wrote a post about flying blind to nowhere and another at the beginning of April discussing what the next few months look like. They were a little bleak, but they have held up to what we are observing in the reported numbers today.
I used an analogy that the USA was a boat in the middle of the ocean. Our boat sinks and we must get into a life raft and then make our way to the shore. The shore being the point of where life is back to normal (immune). At the time I wrote that post (April 2nd), I mentioned we were still swimming to the life raft. As of today, it appears that most of the USA is now in the life raft. We have stabilized infections, hospitalizations, and deaths in most areas of the country.

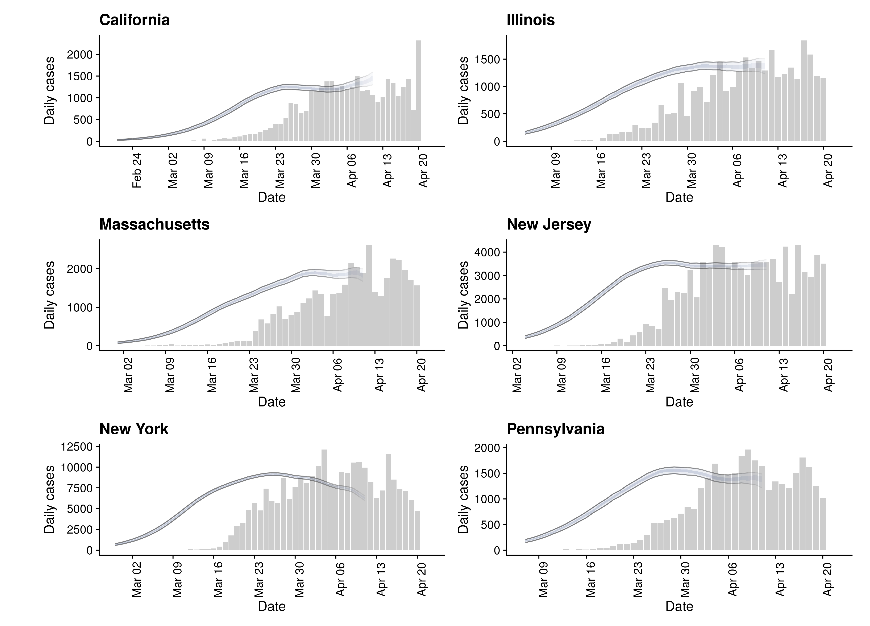
Of the 6 states expected to have the most cases in the next week, New York has finally found the peak, and is on the other side. Illinois, New Jersey, Pennsylvania, California, and Massachusetts are stabilizing in cases. Mortality will lag a week or two, so expect high numbers from those states for a while.
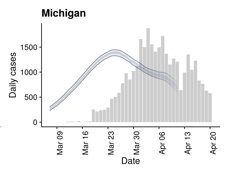
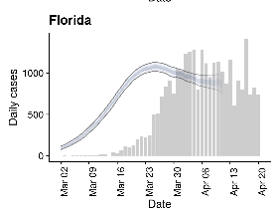
Michigan and Florida were ramping up quickly in infections, and I was concerned. Fortunately they have done remarkably well in finding the other side of their peaks. A big part of these declines have been the testing. Especially in Florida, where they have performed a huge number of tests considering the size of their outbreak. But notice the difference in the backside of the peaks of Florida and Michigan. Michigan is dropping quickly (1500 to 500) while Florida is trending down more slowly. The difference is the stay-at-home compliance.
But all states pale in comparison to Australia, New Zealand, and South Korea, who have been able to turn around their respective peaks quickly. The difference between these countries and the USA is testing, isolation, contact tracing, and quarantine. They have done an extraordinary amount of testing per capita, and their contact tracing has been excellent. In Australia and NZ, everyone listened to the scientists, threw aside politics and just did their job. A great article describing Australia and NZ success can be accessed here. They will be essentially free of COVID-19 within a month, I encourage you to read it.


A key point to Australia's success has been the volume of testing. Their positive to negative rate was 2 positive for every 98 negative tests (2%), and the estimates are that they are identifying >93% of all COVID-19 cases. This aggressive testing, along with the lock down (in Australia and NZ... notice the difference with the lack of stay at home with Korea, the tail hangs on and on), stopped people with the virus spreading it to new hosts.
I know you have heard it from me before, but the testing piece is crucial. You must identify the infected and get them isolated quickly. The longer they stay in the community, the more opportunities they have to spread this virus to others. The optimum is 2-5% percent positive, any lower and you are testing too much, any higher and you are not capturing enough of the new infections to slow the outbreak.
If you look at some states in the USA, 50% of all tests in NJ are positive, while in MA we have 20%, and RI is roughly 15% positive rate (see below). So Massachusetts needs to increase testing 4-5 fold, and NJ at least 10 fold, and RI 3 fold. Without this increase in testing, stronger restrictions need to be enforced to contain the spread of the virus.
I will say it a thousand times, if we don't improve testing capacity, we stay locked down.


This brings me to how each State reopens.
The Federal Government released a 3-phase plan of how to reopen safely. And it's not a bad plan, if followed. Some states will follow, some states won't. So we are about to run a national experiment where the data recorded is how many people die (yes, that is really messed up).
Currently we are in Phase 0. Stay at home advisory, essential workers only.
If we can meet the requirements of entering Phase 1
We can do the following:
Return to work in phases, but telework is still encouraged. States decide which businesses are the most essential.
Gyms can open (Seriously, WTF)
Some restaurants, movie theaters, sports venues, and places of worship can open with strict capacity limits. (Again, WTF)
Hospitals can resume elective procedures
* indoor enclosed environments, where you are in close contact with people, account for 85% of ALL infections. These decisions were political lobbying efforts, not based on biology.
We can't do the following:
Schools remain closed
No visiting senior living facilities
No organized youth sports
The criteria for a state to move into Phase 1. The state must demonstrate the following:
A sustained 14 day decline in new cases of COVID-19 (which has to occur with flat or increasing testing)
A decline in hospitalizations
The state must have the ability to ramp up contact tracing
The state must have the ability to treat all patients without expanded crisis care (e.g. no patients in University Gyms)
Clearly, some states are ignoring the plan. They have chosen to be the control group for the country. For your own state, look here
But, I would like to focus closer to home, where the New England states will take a measured approach. To enter Phase 1, we need to have a sustained decline in hospitalizations and new cases for at least 2 weeks. This is where we stand.
Massachusetts
Cases: Flattening, but no peak yet.
Intensive Care (ICU). Rising. We have roughly 1200 ICU beds in the state (more with surge capacity). As of today, 1034 of them are occupied, up from 973 a week ago. This is concerning and we need this to come down substantially.
Hospitalized: Rising. We have roughly 11,000 hospital beds in the state. We have 2,500 COVID-19 patients in them and 6,400 other patients with other ailments in those beds. So we have some room to spare, plus the additional surge capacity beds in gyms and conference centers.
Rhode Island
New Cases: Rising
ICU: Rising. 75 cases, 45 on ventilators. This is still rising, but currently well below state ICU capacity.
Hospitalized: Rising. 267 cases. Well below hospital capacity.
So, overall, this sucks. Despite all of our personal efforts over the last month, our current level of stay-at-home has not been able to limit the spread to a point where case numbers begin to decline. This should have happened in the first week of April, roughly 2 weeks after the stay-at-home orders were given (like in Michigan and Australia). It suggests that we have both in-house infections and substantial infections happening in the community (via essential employees and by people ignoring the stay-at-home orders/advisory).
This puts us in the status quo for longer, or possibly gives the state Governors evidence they need to increase restrictions further (shelter in place?). We have to turn the numbers around AND clear up the beds, before we can ease our way into Phase 1. That we are nearing ICU bed capacity is the most concerning in MA.
So I'm mad.
I have a lot of blame I can assign to those individuals within the community and those state and federal agencies that have let us down. But I'm not going to point fingers and I'm not going to get political, because this is a biological problem and no amount of finger pointing about past events is going to help resolve the issue.
We, us, you...... are obviously incapable of stopping ourselves from being infected, so the state has to step up and take more responsibility. And here's what they are doing:
Testing: There is great news on the testing front. New PCR tests that use swabs from the front of the nose and even saliva tests are now available. This dramatically reduces the PPE and long-swab requirements for sampling that were slowing us down. This means sampling can increase dramatically, and it is!
In the past 3 days we have seen a huge increase in testing in Massachusetts. We were averaging 5000 tests a day for most of April, we have now jumped to 13,500 tests a day! We have capacity to get to a total of 20,000 tests per day in the state. This gets us close to where we need to be on the testing front for MA. (Happy dance if we can sustain or increase further).
Contact tracing: MA is ramping up contact tracing. 650 new contact tracers have been employed, and they are looking for 350 more. Also, fantastic news. If they contact you, answer the damn phone!
These two acts alone will have a positive effect on the state. It means we can get more infected people and their close contacts off the street. In the short term, we are going to see many more daily cases, this will kill our daily case-curve for about 2 weeks, but then it should drop quickly. We just need to do our part.... stay at home.
Policy based solely on BIOLOGY
April 24th - May 7th: Nothing changes for any of us. Expect many new cases, possibly double what we currently have. This is not cause for concern, just the increased testing will lead to a better capture of positives in the population. Hospitalization numbers should start to stabilize and they are the key measure to watch. They should flatten, and may start dropping during this time.
May 7th - May 15th: Most restrictions stay in place, some restrictions ease if hospitalizations come down. Daily case numbers should substantially drop during this time. The key pieces here are daily cases (dropping quickly), hospitalizations (dropping quickly), and ICU bed space opening up.
May 15th - May 30th: I expect we enter Phase 1. This will be a hard phase for all of us. We will have some normalcy. But social distancing, face masks, store and work place capacity limits will all be requirements. If we get a rebound in cases, more than we can handle with our hospitals, we shut down again.
My big hope here is 2 fold: There are some new treatments in the pipeline that I am pretty excited about, but I don't want my excitement for their prospects to get ahead of the science. I will keep you posted if the data is good. Better treatments keep mild cases out of hospital and moderate cases out of the ICU. Better treatments means you can worry less about increasing daily cases.
My second hope (not supported by any data yet, but I am allowed to have hope when my hope doesn't kill you ), is that "seasonal forcing" will have a modest effect on transmissibility of the virus. Increased heat and sunlight may slow down community transmission outdoors. Again, we don't know if seasonal forcing will come into play, we can just have hope here that it does.
Pray for a hot and humid summer and a fragile virus!
June: If the stars align, and we don't see a rebound in cases from the Phase 1 opening, we can enter Phase 2.
That means:
Most business can reopen, but telework still encouraged.
Still social distancing
Non-essential travel can resume
Camps and schools can resume
Organized sports can resume (minus spectators)
This is based on biological gating parameters. Our state infection numbers need to come way way down. In the hundreds per day with the increased testing. The data will dictate what we SHOULD do, at some stage soon POLITICS will dictate what we will do. I hope they align.
Please stay vigilant in your social distancing and hand/face hygiene efforts. Our behavior over the next 6 weeks dictates what our summer looks like. Wear a mask when in public, especially, in enclosed spaces or in open spaces where you can't maintain appropriate physical space (e.g. sidewalks). If you feel sick, stay home and limit your contact with family members. Get outside, get some sun, get some exercise. There is such a low risk of infection in outdoor open spaces, but the benefits are enormous. The more people buy into this, the quicker the numbers drop, the less anxiety people will feel, and the sooner we can get back to work and support our local businesses.
Please take personal responsibility and maintain social conscience.
Be well!
Erin S. Bromage, Ph.D., is an Associate Professor of Biology at the University of Massachusetts Dartmouth. Dr. Bromage graduated from the School of Veterinary and Biomedical Sciences James Cook University, Australia where his research focused on the epidemiology of, and immunity to, infectious disease in animals. His Post-Doctoral training was at the College of William and Mary, Virginia Institute of Marine Science in the Comparative Immunology Laboratory of late Dr. Stephen Kaattari.
Dr. Bromage’s research focuses on the evolution of the immune system, the immunological mechanisms responsible for protection from infectious disease, and the design and use of vaccines to control infectious disease in animals. He also focuses on designing diagnostic tools to detect biological and chemical threats in the environment in real-time.
Dr. Bromage joined the Faculty of the University of Massachusetts Dartmouth in 2007 where he teaches courses in Immunology and Infectious disease, including a course this semester on the Ecology of Infectious Disease which focused on the emerging SARS-CoV2 outbreak in China.

ClashRoyale is a real-time multiplayer game starring the Royales, your favourite Clash characters and much, much more. Collect and upgrade dozens of cards featuring the clash royale download pc free troops, spells and defenses you know and love, as well as the Royales: Princes, Knights, Baby Dragons and more.
Get looking for the can you Do My Essay service so you are on the right place.
When you are in huge trouble it is good for you to take help of black magic expert astrologer whose mantras does miracles for yoy by resolving troubles
http://www.blackmagicexpertastrologer.com/
Hi Dr. Bromage,
Thank you for all your work and information. I am at a loss to find guidelines for immunosuppressed. I have Crohn’s disease and take immunosuppressives and am “elderly” and live in a highly comtaminated Suburb of NYC. What are my guidelines? Can’t find any guidance anywhere. Would so appreciate any guidance. Thank you.
Just discovered this blog and I am so grateful for this excellent information. Thank you! We live in Florida and have been isolating since mid March and have cancelled all travel plans for the foreseeable future. Now we are starting to think about how to start to be "out" again. All your information is so helpful in trying to figure out what this can safely look like.