The Risks - Know Them - Avoid Them
- Erin Bromage

- May 6, 2020
- 12 min read
Updated: Dec 28, 2021
It seems many people are breathing some relief, and I’m not sure why. An epidemic curve has a relatively predictable upslope and once the peak is reached, the back slope can also be predicted. We have robust data from the outbreaks in China and Italy, that shows the backside of the mortality curve declines slowly, with deaths persisting for months. Assuming we have just crested in deaths at 70k, it is possible that we lose another 70,000 people over the next 6 weeks as we come off that peak. That's what's going to happen with a lockdown.
As states reopen, and we give the virus more fuel, all bets are off. I understand the reasons for reopening the economy, but I've said before, if you don't solve the biology, the economy won't recover.
There are very few states that have demonstrated a sustained decline in numbers of new infections. Indeed, as of May 3rd the majority are still increasing and reopening. As a simple example of the USA trend, when you take out the data from New York and just look at the rest of the USA, daily case numbers are increasing. Bottom line: the only reason the total USA new case numbers look flat right now is because the New York City epidemic was so large and now it is being contained.

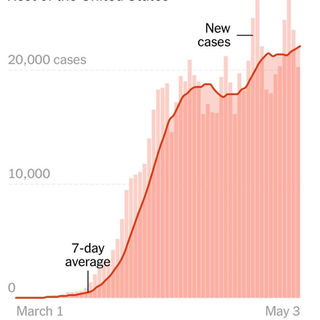
(as of May 3rd)
So throughout most of the country we are going to add fuel to the viral fire by reopening. It's going to happen if I like it or not, so my goal here is to try to guide you away from situations of high risk.
Where are people getting sick?
We know most people get infected in their own home. A household member contracts the virus in the community and brings it into the house where sustained contact between household members leads to infection.
But where are people contracting the infection in the community? I regularly hear people worrying about grocery stores, bike rides, inconsiderate runners who are not wearing masks.... are these places of concern? Well, not really. Let me explain.
In order to get infected you need to get exposed to an infectious dose of the virus; based on infectious dose studies with other coronaviruses, it appears that only small doses may be needed for infection to take hold. Some experts estimate that as few as 1000 SARS-CoV2 infectious viral particles are all that will be needed (ref 1, ref 2). Please note, this still needs to be determined experimentally, but we can use that number to demonstrate how infection can occur. Infection could occur, through 1000 infectious viral particles you receive in one breath or from one eye-rub, or 100 viral particles inhaled with each breath over 10 breaths, or 10 viral particles with 100 breaths. Each of these situations can lead to an infection.
How much Virus is released into the environment?
A Bathroom: Bathrooms have a lot of high touch surfaces, door handles, faucets, stall doors. So fomite transfer risk in this environment can be high. We still do not know whether a person releases infectious material in feces or just fragmented virus, but we do know that toilet flushing does aerosolize many droplets. Treat public bathrooms with extra caution (surface and air), until we know more about the risk.
A Cough: A single cough releases about 3,000 droplets and droplets travels at 50 miles per hour. Most droplets are large, and fall quickly (gravity), but many do stay in the air and can travel across a room in a few seconds.
A Sneeze: A single sneeze releases about 30,000 droplets, with droplets traveling at up to 200 miles per hour. Most droplets are small and travel great distances (easily across a room).
If a person is infected, the droplets in a single cough or sneeze may contain as many as 200,000,000 (two hundred million) virus particles which can all be dispersed into the environment around them.
A breath: A single breath releases 50 - 5000 droplets. Most of these droplets are low velocity and fall to the ground quickly. There are even fewer droplets released through nose-breathing. Importantly, due to the lack of exhalation force with a breath, viral particles from the lower respiratory areas are not expelled.
Unlike sneezing and coughing which release huge amounts of viral material, the respiratory droplets released from breathing only contain low levels of virus. We don't have a number for SARS-CoV2 yet, but we can use influenza as a guide. Studies have shown that a person infected with influenza can releases up to 33 infectious viral particles per minute. But I'm going to use 20 to keep the math simple.
Remember the formula: Successful Infection = Exposure to Virus x Time
If a person coughs or sneezes, those 200,000,000 viral particles go everywhere. Some virus hangs in the air, some falls into surfaces, most falls to the ground. So if you are face-to-face with a person, having a conversation, and that person sneezes or coughs straight at you, it's pretty easy to see how it is possible to inhale 1,000 virus particles and become infected.
But even if that cough or sneeze was not directed at you, some infected droplets--the smallest of small--can hang in the air for a few minutes, filling every corner of a modest sized room with infectious viral particles. All you have to do is enter that room within a few minutes of the cough/sneeze and take a few breaths and you have potentially received enough virus to establish an infection.
But with general breathing, 20 viral particles minute into the environment, even if every virus ended up in your lungs (which is very unlikely), you would need 1000 viral particles divided by 20 per minute = 50 minutes.
Speaking increases the release of respiratory droplets about 10 fold; ~200 virus particles per minute. Again, assuming every virus is inhaled, it would take ~5 minutes of speaking face-to-face to receive the required dose.
The exposure to virus x time formula is the basis of contact tracing. Anyone you spend greater than 10 minutes with in a face-to-face situation is potentially infected. Anyone who shares a space with you (say an office) for an extended period is potentially infected. This is also why it is critical for people who are symptomatic to stay home. Your sneezes and your coughs expel so much virus that you can infect a whole room of people.
What is the role of asymptomatic people in spreading the virus?
Symptomatic people are not the only way the virus is shed. We know that at least 44% of all infections--and the majority of community-acquired transmissions--occur from people without any symptoms (asymptomatic or pre-symptomatic people). You can be shedding the virus into the environment for up to 5 days before symptoms begin.
Infectious people come in all ages, and they all shed different amounts of virus. The figure below shows that no matter your age (x-axis), you can have a little bit of virus or a lot of virus (y-axis). (ref)


The amount of virus released from an infected person changes over the course of infection and it is also different from person-to-person. Viral load generally builds up to the point where the person becomes symptomatic. So just prior to symptoms showing, you are releasing the most virus into the environment. Interestingly, the data shows that just 20% of infected people are responsible for 99% of viral load that could potentially be released into the environment (ref)
So now let’s get to the crux of it. Where are the personal dangers from reopening?
When you think of outbreak clusters, what are the big ones that come to mind? Most people would say cruise ships. But you would be wrong. Ship outbreaks, while concerning, don’t land in the top 50 outbreaks to date.
Ignoring the terrible outbreaks in nursing homes, we find that the biggest outbreaks are in prisons, religious ceremonies, and workplaces, such as meat packing facilities and call centers. Any environment that is enclosed, with poor air circulation and high density of people, spells trouble.
Some of the biggest super-spreading events are:
Meat packing: In meat processing plants, densely packed workers must communicate to one another amidst the deafening drum of industrial machinery and a cold-room virus-preserving environment. There are now outbreaks in 115 facilities across 23 states, 5000+ workers infected, with 20 dead. (ref)
Weddings, funerals, birthdays: 10% of early spreading events
Business networking: Face-to-face business networking like the Biogen Conference in Boston in late February.
As we move back to work, or go to a restaurant, let’s look at what can happen in those environments.
Restaurants: Some really great shoe-leather epidemiology demonstrated clearly the effect of a single asymptomatic carrier in a restaurant environment (see below). The infected person (A1) sat at a table and had dinner with 9 friends. Dinner took about 1 to 1.5 hours. During this meal, the asymptomatic carrier released low-levels of virus into the air from their breathing. Airflow (from the restaurant's various airflow vents) was from right to left. Approximately 50% of the people at the infected person's table became sick over the next 7 days. 75% of the people on the adjacent downwind table became infected. And even 2 of the 7 people on the upwind table were infected (believed to happen by turbulent airflow). No one at tables E or F became infected, they were out of the main airflow from the air conditioner on the right to the exhaust fan on the left of the room. (Ref)


Workplaces: Another great example is the outbreak in a call center (see below). A single infected employee came to work on the 11th floor of a building. That floor had 216 employees. Over the period of a week, 94 of those people became infected (43.5%: the blue chairs). 92 of those 94 people became sick (only 2 remained asymptomatic). Notice how one side of the office is primarily infected, while there are very few people infected on the other side. While exact number of people infected by respiratory droplets / respiratory exposure versus fomite transmission (door handles, shared water coolers, elevator buttons etc.) is unknown. It serves to highlight that being in an enclosed space, sharing the same air for a prolonged period increases your chances of exposure and infection. Another 3 people on other floors of the building were infected, but the authors were not able to trace the infection to the primary cluster on the 11th floor. Interestingly, even though there were considerable interaction between workers on different floors of the building in elevators and the lobby, the outbreak was mostly limited to a single floor (ref). This highlights the importance of exposure and time in the spreading of SARS-CoV2.


Choir: The community choir in Washington State. Even though people were aware of the virus and took steps to minimize transfer; e.g. they avoided the usual handshakes and hugs hello, people also brought their own music to avoid sharing, and socially distanced themselves during practice. They even went to the lengths to tell choir members prior to practice that anyone experiencing symptoms should stay home. A single asymptomatic carrier infected most of the people in attendance. The choir sang for 2 1/2 hours, inside an enclosed rehearsal hall which was roughly the size of a volleyball court.
Singing, to a greater degree than talking, aerosolizes respiratory droplets extraordinarily well. Deep-breathing while singing facilitated those respiratory droplets getting deep into the lungs. Two and half hours of exposure ensured that people were exposed to enough virus over a long enough period of time for infection to take place. Over a period of 4 days, 45 of the 60 choir members developed symptoms, 2 died. The youngest infected was 31, but they averaged 67 years old. (corrected link)
Indoor sports: While this may be uniquely Canadian, a super spreading event occurred during a curling event in Canada. A curling event with 72 attendees became another hotspot for transmission. Curling brings contestants and teammates in close contact in a cool indoor environment, with heavy breathing for an extended period. This tournament resulted in 24 of the 72 people becoming infected. (ref)
Birthday parties / funerals: Just to see how simple infection-chains can be, this is a real story from Chicago. The name is fake. Bob was infected but didn't know. Bob shared a takeout meal, served from common serving dishes, with 2 family members. The dinner lasted 3 hours. The next day, Bob attended a funeral, hugging family members and others in attendance to express condolences. Within 4 days, both family members who shared the meal are sick. A third family member, who hugged Bob at the funeral became sick. But Bob wasn't done. Bob attended a birthday party with 9 other people. They hugged and shared food at the 3 hour party. Seven of those people became ill.
But Bob’s transmission chain wasn’t done. Three of the people Bob infected at the birthday went to church, where they sang, passed the tithing dish etc. Members of that church became sick. In all, Bob was directly responsible for infecting 16 people between the ages of 5 and 86. Three of those 16 died.
The spread of the virus within the household and back out into the community through funerals, birthdays, and church gatherings is believed to be responsible for the broader transmission of COVID-19 in Chicago. (ref)
Sobering right?
Commonality of outbreaks
The reason to highlight these different outbreaks is to show you the commonality of outbreaks of COVID-19. All these infection events were indoors, with people closely-spaced, with lots of talking, singing, or yelling. The main sources for infection are home, workplace, public transport, social gatherings, and restaurants. This accounts for 90% of all transmission events. In contrast, outbreaks spread from shopping appear to be responsible for a small percentage of traced infections. (Ref)
Importantly, of the countries performing contact tracing properly, only a single outbreak has been reported from an outdoor environment (less than 0.3% of traced infections). (ref)
So back to the original thought of my post.
Indoor spaces, with limited air exchange or recycled air and lots of people, are concerning from a transmission standpoint. We know that 60 people in a volleyball court-sized room (choir) results in massive infections. Same situation with the restaurant and the call center. Social distancing guidelines don't hold in indoor spaces where you spend a lot of time, as people on the opposite side of the room were infected.
The principle is viral exposure over an extended period of time. In all these cases, people were exposed to the virus in the air for a prolonged period (hours). Even if they were 50 feet away (choir or call center), even a low dose of the virus in the air reaching them, over a sustained period, was enough to cause infection and in some cases, death.
Social distancing rules are really to protect you with brief exposures or outdoor exposures. In these situations there is not enough time to achieve the infectious viral load when you are standing 6 feet apart or where wind and the infinite outdoor space for viral dilution reduces viral load. The effects of sunlight, heat, and humidity on viral survival, all serve to minimize the risk to everyone when outside.
When assessing the risk of infection (via respiration) at the grocery store or mall, you need to consider the volume of the air space (very large), the number of people (restricted), how long people are spending in the store (workers - all day; customers - an hour). Taken together, for a person shopping: the low density, high air volume of the store, along with the restricted time you spend in the store, means that the opportunity to receive an infectious dose is low. But, for the store worker, the extended time they spend in the store provides a greater opportunity to receive the infectious dose and therefore the job becomes more risky.
Basically, as the work closures are loosened, and we start to venture out more, possibly even resuming in-office activities, you need to look at your environment and make judgments. How many people are here, how much airflow is there around me, and how long will I be in this environment. If you are in an open floorplan office, you really need to critically assess the risk (volume, people, and airflow). If you are in a job that requires face-to-face talking or even worse, yelling, you need to assess the risk.
If you are sitting in a well ventilated space, with few people, the risk is low.
If I am outside, and I walk past someone, remember it is “dose and time” needed for infection. You would have to be in their airstream for 5+ minutes for a chance of infection. While joggers may be releasing more virus due to deep breathing, remember the exposure time is also less due to their speed. Please do maintain physical distance, but the risk of infection in these scenarios are low. Here is a great article in Vox that discusses the low risk of running and cycling in detail.
While I have focused on respiratory exposure here, please don't forget surfaces. Those infected respiratory droplets land somewhere. Wash your hands often and stop touching your face!
As we are allowed to move around our communities more freely and be in contact with more people in more places more regularly, the risks to ourselves and our family are significant. Even if you are gung-ho for reopening and resuming business as usual, do your part and wear a mask to reduce what you release into the environment. It will help everyone, including your own business. This article was inspired by a piece written by Jonathan Kay in Quillete
About the author
Erin S. Bromage, Ph.D., is an Associate Professor of Biology at the University of Massachusetts Dartmouth. Dr. Bromage graduated from the School of Veterinary and Biomedical Sciences James Cook University, Australia where his research focused on the epidemiology of, and immunity to, infectious disease in animals. His Post-Doctoral training was at the College of William and Mary, Virginia Institute of Marine Science in the Comparative Immunology Laboratory of late Dr. Stephen Kaattari.
Dr. Bromage’s research focuses on the evolution of the immune system, the immunological mechanisms responsible for protection from infectious disease, and the design and use of vaccines to control infectious disease in animals. He also focuses on designing diagnostic tools to detect biological and chemical threats in the environment in real-time.
Dr. Bromage joined the Faculty of the University of Massachusetts Dartmouth in 2007 where he teaches courses in Immunology and Infectious disease, including a course this semester on the Ecology of Infectious Disease which focused on the emerging SARS-CoV2 outbreak in China.

Hi there You overseas! I am from Hungary/Europe. We hear you have exploding numbers of Omicron infections. Is this the real situation?
Is it correct that Professor Bromage hasn't posted in over a year and a half? I would very much like to see a more recent assessment of the Covid situation from his viewpoint. I was very fascinated by his original postings.
It is amusing to see the Charles Koch operatives at work. It is a clear indication that Dr Bromage’s Blog has scared Charles Koch enough to begin attacking it a year latter with a troll.
My advice,; Don’t feed the trolls!
Is there a way to report laurie0420? She's posting dangerous nonsense here. I hope there's a way that Dr. Bromage can remove her posts and ban her from commenting here.
How is this article recycling and why am I getting notifications of trolls posting nonsense?